Pharmacology and classification of opioid analgesics
Opioids are medications. Pharmacology of opioid analgesics
Given the centuries-old history of the use of opium and its alkaloids, it was only in 1973 that the presence of membrane receptors called “opioids” in the central nervous system was experimentally proven. A little later, it was possible to detect in the body the first substance stimulating endogenous opioid receptors, called enkephalin (from the word “kephale” – head). Currently, there are 3 families of endogenous opioids.:
endorphins
, enkephalins
, and dynorphins.
All endogenous opioid peptides are formed from protein precursors produced in various proportions in parts of the nervous system and peripheral organs. At the same time, along with pain suppression, endogenous opioids participate in the regulation of the functions of the gastrointestinal tract, endocrine glands, heart, higher nervous activity, etc. The biological effects of endogenous opioids are realized by stimulating opioid receptors localized in both the central nervous system and peripheral tissues. At least five types of receptors are currently known.:
μ (mu) – receptors
k (kappa) – receptors
δ (delta) – receptors
σ (sigma) – receptors
e (epsilon) – receptors.
Each of these types has a specific location and physiological significance (Table 16). Meanwhile, the main physiological task of opioid receptors is to maintain adequate antinoception by suppressing the functions of the nociceptive system.
Heroin or diamorphine is a semi-synthetic opioid drug used as a medicinal product in the late 19th and early 20th centuries. Its use leads to such harmful effects as vein rupture, pneumonia, hepatitis, infectious diseases and abscesses, as well as severe depression.
Opium is a powerful narcotic that is extracted from the sun-dried milky juice of unripe opium poppy pods. It was used as a strong painkiller, but quickly caused drug dependence and today is used only as a raw material for the production of painkillers (morphine, codeine, papaverine and others), as well as for the synthesis of the drug heroin.
Oxycontin, a drug that was considered the most effective painkiller, especially for cancer, has the same effect on humans as heroin when the dose is increased.

Painkillers containing opiates
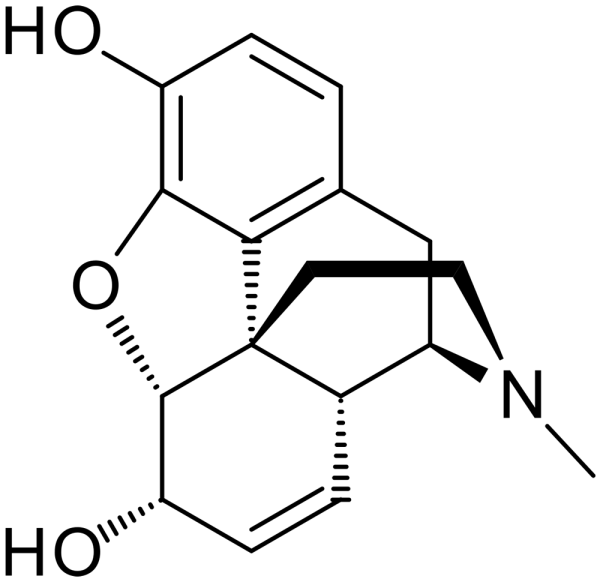
Morphine is one of the main alkaloids of opium, found in poppy as a sleeping pill. It is sold in various forms, such as Roxanol medicine or long-acting tablets MS-contin – Morphine sulfate. It acts on brain receptors and is quite addictive, so when taking it, you should strictly adhere to the dose recommended by your doctor. In high doses, it has a strong hypnotic effect. Slows down conditioned reflexes.
Codeine is similar in nature to morphine, but its analgesic properties are weaker. It is used for moderate pain. It is often prescribed in combination with the painkiller Tyrenol, it is quite addictive, so when taken, you must strictly adhere to the dose recommended by your doctor.
Vicodin (Vicodan, Lortab, Lorcet) is a powerful narcotic analgesic and antitussive medicine. The combination of Acetaminophen (Tyrenol) and Hydrocodone acts on brain receptors and prevents the production of the hormone prostaglandin, which causes pain, and is prescribed for moderate to severe pain.
Norco (Digiroxycodeine, Dicophene, Lexia, Tylox, Pentalgin) is an analgesic drug, a combination of Acetaminophen (Tyrenol) and Hydrocodone, acts on brain receptors and prevents the production of the hormone prostaglandin, which causes pain, is prescribed for moderate to severe pain. It is quite addictive, so when taking it, you must strictly adhere to the dose recommended by your doctor.
Methadone is a synthetic drug from the group of opioids used as an analgesic, as well as in the treatment of drug addiction. A strong painkiller. Methadone addiction is difficult to cure because Methadone has a prolonged effect on the body and persists in the tissues for a long time.
Stadol is an opioid analgesic, similar to morphine in terms of its analgesic effect. It is prescribed for those who have undergone surgery or suffer from migraines. It is most common in the form of nasal spray. It is quite addictive, so when taking it, you must strictly adhere to the dose recommended by your doctor.
LAAM (LAAM, Levacetylmethadol) is an analgesic used in the substitution therapy of opioid addiction: LAAM does not treat addiction. but it helps the patient to cope with “withdrawal symptoms” after stopping taking opiate drugs.
Percocet (Oxycodone, Percodan) – the pharmacological profile of Percocet is the same as that of morphine. Like codeine and hydrocodone, Percocet is well absorbed after oral administration, providing an analgesic effect for at least half an hour. It acts on brain receptors and prevents the production of the hormone prostaglandin, which causes pain. It is quite addictive, so when taking it, you must strictly adhere to the dose recommended by your doctor.
Dilauid (Hydromorphone) is distributed in the form of tablets and liquid for injection. Its effectiveness as an analgesic is two to eight times higher than that of morphine. This feature makes the use of hydromorphone especially advisable in patients with renal insufficiency. In other respects, hydromorphone is practically the same as morphine.
Hydrocodone is a cough suppressant, an opioid analgesic, a very popular remedy, the production of which has increased 4 times over the past decade. It causes rapid physical and psychological dependence, so do not exceed the prescribed dose, and if stopped abruptly, it can cause withdrawal symptoms.
Darvocet is an analgesic drug that was very popular in the United States and Great Britain just a few years ago, containing the narcotic component Propoxyphene, which acts on brain receptors. In 2010, it was discontinued and banned by law in the United States, as it has a negative effect on the cardiovascular system.
Tramadol is prescribed for severe pain after surgery or chronic diseases such as arthritis. Reduces the body’s sensitivity to pain. It is quite addictive, so when taking it, you must strictly adhere to the dose recommended by your doctor.
Suboxone (Buprenorphine) is a semi-synthetic opioid, a powerful painkiller. It causes a stronger analgesic effect than morphine and methadone, but less euphoria.
Tramal (Tramadol) is an analgesic opioid drug with central action and action on the spinal cord. Tramal has a sedative effect and depresses the respiratory center. With prolonged use, tolerance may develop and a dose increase is required.
Narcotic analgesic drugs are opiates, substances of the morphine group that affect the central nervous system and lower the pain threshold, as well as change the emotional perception of pain. Opioid narcotic analgesics are so named due to the fact that after repeated use they cause dependence, both physical and mental, in the common people – drug addiction.
Opioid analgesic – all opium derivatives, both natural and synthetic. It is these narcotic drugs that can have an analgesic effect and affect such receptors.:
Delta receptors (opioid receptor agonists – leu enkephalin and megenkephalin).
Kappa (stimulating these receptors can suppress the production of dopamine).
Mu receptors (opioid receptor agonists – morphine and fentanyl).
The main alkaloid of opium is morphine. Non-natural, similar narcotic drugs have a similar pharmacological mechanism, but they contain other compounds. Next, we will tell you how this analgesic narcotic drug works, what the indications for its use may be, and also describe the possible side effects after using such therapy.
The classification of opioid analgesics, depending on the degree of effect of the narcotic drug on the receptors, divides opium derivatives into the following subgroups::
Partial ones.
Antagonists are agonists.
Full ones.
Drugs of mixed action.
Opioid receptor agonists are the most effective drugs, which are presented in the form of Morphine, Methylmorphine, Methadone, Fentanyl and Promedol. Partial agonists of opioid receptors – ligands are a little weak, because they are not so much and not so strongly related. The most famous representative of this category is Buprenorphine.
An agonist- antagonist of opioid analgesics is able to excite some receptors, while others, on the contrary, slow down. The list of drugs in this category includes Pentazocine, Butorphanol and Nalbufin. Naloxone is recognized as an absolute antagonist. Narcotic drugs of mixed effect are opioid analgesics Tramadol.
How do narcotic drugs work?
As we said at the beginning, opioid analgesics act on the nervous system. Also, opioid analgesics, as endogenous opiate peptides, can affect the antinociceptive system and contact the neurons of the gelatinous substance in the spinal cord. In addition to the hormone endorphin, serotonin and glycine are involved in this system.
Morphine, like other strong opioid analgesics, for the most part relieves severe pain that comes from the spinal cord on its way to the nuclei of the thalamus, preventing its proliferation in the upper convolutions of the cerebral cortex and hypothalamus, where the body’s reactions to pain are formed. Because of this, psychotropic effects occur in the form of euphoria.:
The feeling of fear and anxiety disappears.
Attention shifts away from unpleasant sensations.
A person experiences indifference to the world around them.
It is precisely because a person wants to experience such sensations again that mental dependence on the drug arises. This addiction very often develops in children during adolescence. If you stop using opioid analgesics, you can observe:
Vegetative disorders (lacrimation, increased perspiration, dilated pupils, nausea, vomiting and diarrhea).
Problems with the cardiovascular system (spikes in blood pressure, tachycardia).
Mental disorders (poor sleep, hallucinations).
Such and other manifestations can accompany a person for about 3 days. Drug addicts will go to great lengths to eliminate them, but only to get the necessary dose of the drug. With regular abuse of opioid analgesics, a person degrades.

Indications for the use of narcotic painkillers
Opioid and non-opioid analgesics are prescribed to both children and adults in this case.:
To relieve pain from various injuries and burns.
To eliminate postoperative pain syndrome.
To minimize pain during painful manipulations.
In case of severe pain due to ureteral spasm, etc.
For the treatment of children with malignant neoplasms that do not respond to surgical intervention.
During the acute period of myocardial infarction.
With shortness of breath and pulmonary edema.
For pain relief of labor.
When hepatic colic occurs.
Please note that opioid analgesics Tramadol, Morphine and other analogues improve the patient’s mental state much more effectively than non-narcotic analgesics.
To enhance the effects of opioid analgesics, they are very often combined with tranquilizers or antipsychotics. This combination, as a rule, complements each other, and in cases with children, it can completely replace anesthesia. In this way, the child does not pay attention to the pain and becomes indifferent to everything that is happening around him. But that’s not all. In the treatment of infants and children under 2 years of age, nitrous oxide and oxygen are additionally used in a 1:1 ratio.
Possible side effects and contraindications from the use of narcotic drugs
I would like to immediately draw your attention to the fact that opioid analgesics Tramadol and its narcotic derivatives, as well as stronger narcotic drugs, should not be used for more than 4 days, otherwise it will not be possible to avoid dependence (drug addiction) in the patient. Contraindications that do not allow the use of opioid analgesics Tramadol, Morphine, Methadone, and other narcotic drugs include:
Depressed breathing.
Bronchial asthma.
Various head, brain, and other injuries, which are accompanied by increased intracranial pressure;
Pregnancy.
Childbirth.
Children whose age has not reached the age of 2 years.
This category of narcotic drugs is unacceptable for traumatic brain injuries, because as a result of depressed breathing and accumulation of carbonic acid, vasodilation occurs in the brain, which increases the risk of edema. Side effects can also look like:
Central nervous system depression.
Loss of consciousness.
Depressed breathing.
Drop in blood pressure.
Constricted pupils that do not respond to changes in light brightness.
Tonic-clonic seizures.
To get rid of intoxication from the drug Morphine and its derivatives, the most effective way is to introduce antagonists that eliminate the effects of the narcotic drug and help restore the normal functioning of the central nervous system. If you suddenly do not have antagonists, you can use analeptics that do not cause seizures, or caffeine. If there is a deep respiratory depression, artificial ventilation of the lungs will have to be performed.
How to deal with poisoning from a narcotic analgesic drug?
Acute poisoning is the result of an overdose of narcotic drugs, which occurred both intentionally and unintentionally. The dynamics of changes can be explained in this way:
The very first signal can be seen half an hour after consumption – general weakness, dizziness, vomiting, a desire to sleep, unjustified euphoria abruptly turning into stupor, symmetry with pupil constriction, hypothymia.
The feeling of pain is minimized, the patient falls asleep, and then completely loses consciousness.
Breathing slows down.
Blood pressure drops suddenly, and seizures can be seen in children.
If the outcome of the disease is favorable, the coma will turn into a normal sleep in just a day and a half. In the unfavorable case, death will occur in 18 hours (maximum), which will be accompanied by paralysis of the respiratory center and respiratory failure. But such adverse effects can be avoided by restoring breathing or maintaining it in this way.:
By transferring the patient to an artificial lung ventilation system.
By performing antidote detoxification by injecting Naloxone intravenously.
Repeat gastric lavage with a probe or activated charcoal.
What’s it?
Opioids are all synthetic and natural substances that are able to establish a connection with the opioid receptors of the body, which are located in the gastrointestinal tract and central nervous system: stimulate and block them.
What are opioids? First of all, these are the most powerful pain relievers. In addition to the sedative and analgesic effect, they can also weaken intestinal motility, depress the cough and respiratory center.
They should not be confused with opiates (Latin opium is a strong drug that is produced from dried milky juice extracted from unripe opium poppy pods). This type includes only natural substances extracted from the poppy. These are thebaine, morphine, oripavine, codeine, etc. Thus, opiates can also be opioids, while opioids are not always opiates, as they also have a synthetic structure.
The main disadvantage of opiates and opioids is the ability to cause a person to feel euphoric. Because of this, some people do not use opioids for medicinal purposes. This addiction leads to addiction and subsequent withdrawal (withdrawal syndrome).
Facts about Opioids
To find out what opioids are, this collection of facts from :
Opioids are psychoactive substances. An example is heroin and morphine.
Every year, 69,000 people die worldwide due to an overdose of these drugs.
The average number of people suffering from opioid addiction worldwide was 15 million. However, not all of them use illegal heroin. Many people also use prescription opioids.
Only 10% of addicts receive treatment for their addiction.
The pharmacological effect of opioids is such that when taking a large dose of them, respiratory depression and subsequent death occur.
The consequences of an opioid overdose (including death) can be eliminated by an inexpensive drug called Naloxone.
The negative effect of opioids
The main disadvantage of the drug is the appearance of dependence on opioids. This implies the following:
Strong narcotic desire to use the drug.
Impaired ability to control one’s behavior.
The appearance of harmful consequences.
The loss of the meaning of a normal life in pursuit of the effects of an opioid.
Withdrawal symptoms after discontinuation of medication.
Opioids in history
Humanity knew what opioids were 4 thousand years ago. It is known that in the Minoan civilization, the goddess was especially revered, whose image was surrounded by a crown of opium poppy boxes. Opioids were also known to later civilizations – Corinth (Greece) and Afyon (Turkey). From there, the extraction of opium from poppies spread to the East.
It should be noted that until the middle of the 17th century, opioids were used exclusively as painkillers, and not as a drug. But opium smoking, in a desire to fall into euphoria, began to spread in China in the second half of the 17th century. It is impossible not to recall the so-called Opium Wars that broke out at the end of the XVIII century. The reason for them was that the British East India Company, using its monopoly position, imported huge quantities of opium into China.
1804 – the German pharmacist F. Serturner was able to extract from opium its main active ingredient, named by the discoverer “morphine” (the term “morphine” was introduced a little later by Gay-Lussac).
1898 – semi-synthetic morphine derivatives called “heroin” and “ethylmorphine” entered medical use.
1937 – the first fully synthetic opioid pethidine was produced in Germany. A little later, methadone of the same nature was synthesized. In the Soviet Union, a derivative of pethidine, promedol, was used.
Late 1950s – fentanyl was synthesized in Belgium.
The structure of opioids
The chemical structure of opioids is very diverse. Their most common component is a benzene ring, which is connected by a propyl or ethyl “bridge” to a nitrogen atom. This is what ensures the similarity of opioids to tyrosine, an amino acid that is part of enkephalin (the simplest opioid peptide) and plays an important role in its interaction with opioid receptors.
The nitrogen atom is most often represented here by a component of the piperidine ring. A significant part of opioids are tertiary amines.
Classifications
There are several classifications of opioids:
by origin;
by action;
by structure.
Let’s analyze each of them in detail.

Gradation of opioids by origin
So, opioids. What applies to them in this group? Drugs divided into several more smaller gradations:
Natural, vegetable:
opium poppy alkaloids: thebaine, morphine, codeine;
other herbal opioids: salvinorin A, mitragynine.
Synthetic, artificial: methadone, promedol, tramadol, fentanyl, etc.
Semi-synthetic: heroin, ethylmorphine, hydromorphone, etc.
Endogenous (those that are produced directly by the body itself): endorphin, nociceptin, enkephalin, endomorphin, and dynorphin.
Gradation of opioids by action
Now let’s look at other opioids, what belongs to them according to this classification.:
Antagonists: nalmefene, naloxone, naltrexone.
Partial agonists: oxycodone, propoxyphene, codeine, diphenoxylate, hydrocodone.
Full agonists: heroin, methadone, fentanyl, hydromorphone, oxydone, morphine, alfentanil, oxymorphone, levorphanol, alfentanil, meperidine, remifentanil.
Antagonists-agonists of mixed effect: pentazocine, buprenorphine, nalorphine, nalbufin, butorphanol.
Classification of opioids by structure
Which drugs belong to opioids in this classification? Having the following elements in their composition:
Phenanthrenes (4,5α- epoxymorphinans) are natural or semi-synthetic opioids similar in structure to morphine, i.e. having a piperidine and aromatic ring. These are heroin, codeine, morphine, hydrocone, oxycodone, naloxone, 6-monoacetylmorphine, buprenorphine, nalbufin, oxymorphone.
Morphinans, Their structure differs from that of morphine by the epoxy removed “bridge”. They are also distinguished by their purely synthetic origin. These are dextromethorphan, levorphanol, butorphanol.
Benzomorphans are compounds such as phenazocine, metazocine, and pentazocine.
Diphenylheptanones.
Phenylpiperidines.
4-anyldopiperidines.
Separation by impact
What are these opioid drugs? These are also drugs that differ in the intensity of their effects on the systems of the human body. Within this framework, three groups are distinguished::
Potent drugs: fentanyl, buprenorphine, sufentanil, carfentanil, remifentanil, brifentanil, alfentanil.
Medium-intensity drugs: pentazocine, codeine, trimeperidine, nalbufin.
Weak-acting drugs – for example, tramadol.
Classification of opioid analgesics
Opioid analgesics and their antagonists can be separated:
by chemical structure and origin,
by its effect on opioid receptors.
For a medical practitioner, the second, so-called clinical classification, is indispensable.
By chemical structure and origin
Natural opioid analgesics (phenanthrene derivatives): morphine, codeine.
Synthetic opioid analgesics :
Phenanthrene derivatives: heroin, oxymorphone, hydromorphone, nalbufin, buprenorphine;
Piperidine derivatives: promedol (trimeperidine), meperidine, pyritramide, fentanyl, lofentanyl, carfentanyl, sufentanyl, etc.;
Phenylheptylamines: meptazinol, methadone;
Benzomorphans: pentazocine;
Morphinans: levorphanol, butorphanol, dextromethorphan;
Cyclohexanols: tramadol.
On the effect on opioid receptors
Pure agonists
Strong agonists: morphine, trimeperidine (promedol), meperidine, methadone, fentanyl, etc.;
Weak agonists: codeine, propoxyphene, oxycodone, hydrocodone;
Mixed agonist-antagonists and partial agonists: buprenorphine, butorphanol, pentazocine, tramadol.
Pure opioid receptor antagonists: naloxone, nalmefene, naltrexone, alvimopan, methylnatrexone.
Pure opioid receptor agonists eliminate the effects of opioid analgesics. Naloxone and nalmefene are indispensable for respiratory depression caused by an overdose of opioid analgesics, naltrexone is used in the treatment of opioid addiction and alcoholism. The latter two substances do not penetrate the central nervous system and are used to eliminate opioid-induced constipation.
Mechanism of action of opioid analgesics
Opioid analgesics eliminate pain by stimulating specific opioid receptors that regulate the transmission and modulation of pain and are located primarily in the brain and spinal cord. They inhibit the release of excitatory mediators from afferent neurons and inhibit the transmission of pain impulses in the dorsal horns of the spinal cord, and at the supraspinal level they disrupt the transmission and modulation of pain.
A particularly important point is the modulation of pain in the descending pathways, including the anterior cerebral keel, the gray periaqueductal zone and the locus ceruleus. Opioid analgesics suppress all these neurons and promote the release of endogenous opiopeptides, which, in turn, act on other types of receptors than opioid analgesics themselves. Therefore, there are no analgesics selective for one type of receptor.
Effects of opioid analgesics
The prototype of opioid analgesics is morphine. Other opioid analgesics cause only morphine-like effects. All the effects of morphine can be divided into central and peripheral.
The central effects of morphine
Effects of CNS depression
Analgesia caused by a change in the perception of pain, a change in the reaction to pain (pain is perceived as something extraneous) and euphoria (a strong sense of satisfaction and well-being). Healthy people who do not have pain may sometimes have dysphoria. Strong mu receptor agonists have the most pronounced effect.
Respiratory depression caused by decreased sensitivity of the respiratory center to carbon dioxide. The respiratory rate decreases and in case of overdose, it may stop (death). A decrease in the respiratory rate caused by morphine is useful for shortness of breath accompanying pulmonary edema (the patient’s fear of shortness of breath itself decreases). The accumulation of carbon dioxide during decreased breathing leads to relaxation of cerebral vessels and increased intracranial pressure (and this is dangerous for head injuries).
Suppression of the cough center is not proportional to the analgesic effect. Thus, the weak opioid analgesics codeine and dextromethorphan have a strong antitussive effect.
Sleep , which is explained by the consequence of pain relief – the patient calms down and falls asleep.
Effects of CNS arousal
Vomiting (due to stimulation of the chemoreceptors of the trigger zone of the vomiting center) is more common in patients who are in motion and is not accompanied by unpleasant sensations. There is no vomiting with chronic use.
Miosis (pupil constriction) caused by the stimulating effect of parasympathetic innervation on the tone of the oculomotor nerve nucleus. This effect persists with chronic use (i.e., there is no addiction). Miosis, bradypnosis (rare breathing), and coma are reliable diagnostic symptoms of overdose with opioid analgesics.
Convulsions. This is an extremely rare effect of meperidine and trimepiridine (promedol) when they are overdosed on the background of renal failure due to the accumulation of toxic metabolites.
The rigidity of the trunk muscles reduces the volume of respiratory movements and can disrupt the patient’s breathing. It is most pronounced with rapid intravenous administration of high doses of opioid analgesics with high lipid solubility (fentanyl and related substances). To relieve rigidity (the reason for it is opioid analgesics act at the supraspinal level), curare–like muscle relaxants are prescribed.
Peripheral effects of morphine
Constipation due to suppression of intestinal motility while increasing the tone of the smooth muscles of the large intestine and spasm of the anal sphincter. All this leads to a slowdown in the progress of the chyme (food lump), water absorption and constipation. This effect is widely used in diarrhea of non-infectious origin. Opioid analgesics are considered the most effective group of substances for diarrhea. Loperamide (imodium) and diphenoxylate, which are chemically related to opioid analgesics, are used. They are safe because they do not penetrate the central nervous system and therefore do not cause euphoria, analgesia, or drug addiction.
Spasm of the biliary tract muscles (may cause hepatic colic).
Increased tone of the ureter, detrusor and sphincter of the bladder, which can increase the course and (with prostate adenoma) cause urinary retention.
The cardiovascular system is changed only by substances with an M-holinoblocking effect. For example, trimeperidine (promedol) and meperidine can cause tachycardia. However, opioid analgesics can cause slight hypotension due to the release of histamine and decreased tone of the vasomotor center.
The release of histamine from mast cells leads to vasodilation of the skin, which may lead to a slight decrease in blood pressure. There may also be itching of the skin, urticaria and bronchospasm in asthmatics.
Decreased renal excretory function: decreased renal blood flow and glomerular filtration.
Decreased uterine tone , which can cause labor to slow down. The mechanism of this effect is unknown.
Pharmacokinetics
The vast majority of opioid analgesics are well absorbed into the gastrointestinal tract, then they are metabolized in the liver and excreted in the urine in the form of metabolites (glucuronides, etc.). However, there are differences in the rate and magnitude of absorption in the gastrointestinal tract (therefore, opioid analgesics are most often prescribed parenterally, this is a more accurate method) and the peculiarities of liver metabolism. For example, the administration of a large dose of morphine against the background of kidney damage leads to the accumulation of a neurotoxic metabolite of morphine (morphine-3-glucuronide) in the body, which can cause seizures. A similar effect may occur with the accumulation of metabolites of meperidine or its analogues. With repeated administration of large doses of opioid analgesics (especially those with high lipophilicity, such as fentanyl), they may accumulate in adipose tissue, which creates a risk of toxic effects.
Combinations with opioid analgesics
The depressive effects of opioid analgesics (including analgesia) are enhanced:
neuroleptics (a combination of fentanyl + droperidol is used for neuroleptic analgesia),
sedatives and hypnotics, which increases the risk of respiratory depression.;
Antidepressants – combination with MAO inhibitors is contraindicated due to the risk of hyperpyrexic coma;
Amphetamines paradoxically enhance the analgesia of opioid analgesics.
Comparative characteristics of opioid analgesics
Opioid analgesics differ from each other in terms of duration of action, severity (strength) of individual effects, and risk of drug dependence.
According to the duration of action, opioid analgesics are divided into substances:
short-acting (about 30 minutes), for example, fentanyl;
the average duration of action (about 6 hours), for example, morphine;
long-acting (about 25 hours), for example, methadone.
painkillers: for example, morphine is about 70 times weaker than fentanyl;
smooth muscle spasms: promedol and meperidine have the least, which are similar in structure to atropine.;
Antitussive effect: strong in codeine, very weak in promedol (trimeperidine).
According to the risk of drug dependence, opioid analgesics are divided into substances whose purpose involves:
high-risk drug addicts (strong agonists);
with a low risk of addiction (mixed agonist antagonists and partial agonists). Although they try to give preference to this group if long-term treatment is necessary, their effectiveness is not always sufficient to eliminate pain. In addition, they can cause undesirable mental effects: hallucinations, nightmares, anxiety. When taken simultaneously with strong opioid receptor agonists, they behave like antagonists – that is, they displace the latter from their connection with opioid receptors. At the same time, drug addicts will have withdrawal symptoms, and patients with pain will have reduced analgesia.
without the risk of addiction: antidiarrheal opioids (loperamide, diphenoxylate) and antitussive opioid dextromethorphan. Strictly speaking, the substances in this group are not true opioid analgesics (since they do not cause analgesia), but they are very close to them in chemical structure.
Indications for the use of opioid analgesics
Opioid analgesics are used in the following cases:
Severe acute pain (myocardial infarction, injury, burns, colic) and severe chronic non-inflammatory pain (cancer). Pain relief should be adequate to the severity of the pain and should be reviewed from time to time in the direction of increasing or decreasing dosages. For example, with hepatic or renal colic, pain may increase rather than decrease after opioid administration. This is due to an increase in smooth muscle spasm. Therefore, with colic, it is important to increase the dose of opioids, which will cause effective pain relief. With inoperable cancer, it is even possible to take the risk of creating drug dependence in such patients (high doses of substances, constant administration), but to achieve effective pain relief.
In other cases, preference is given to strong agonists (for acute pain) and partial agonists for chronic pain (due to the low risk of addiction). It should be borne in mind that partial agonists are inferior in effectiveness to strong agonists.
Anesthesia during surgical operations (premedication and immediately during surgery). Fentanyl and its derivatives are especially commonly used.
Pulmonary edema (a decrease in the respiratory rate reduces the patient’s fear) and a decrease in preload and afterload on the heart (due to the expansion of venous and arterial vessels). Morphine is most commonly used.
Pain during childbirth . In the CIS, an analogue of the foreign meperidine is used – trimeperidine (promedol). Compared to morphine, it slightly depresses fetal respiration. In addition, its metabolism (rapid demethylation) is safe for the fetus, compared with the metabolism of morphine (slow conjugation in the liver). Unlike other opioid analgesics, trimeperidine and meperidine do not weaken, but enhance labor activity.
Cough : codeine, dextromethorphan;
Diarrhea (not infectious): diphenoxylate (reasec), loperamide (imodium).
Side effects of opioid analgesics
Opioid analgesics have side effects that are a continuation of their pharmacological action: respiratory depression, constipation, drug dependence, nausea, vomiting, and (toxic doses of trimeperidine, meperidine, tramadol, and less commonly morphine) seizures. Agonists may have psychotomimetic reactions (hallucinations, nightmares, and anxiety).
Contraindications
According to the side effects, opioid analgesics are contraindicated in:
respiratory depression (except for patients on a ventilator);
with an attack of bronchial asthma or with its severe form, even outside the attack;
with paralytic ileus.